Translational Perioperative and Pain Medicine (ISSN: 2330-4871)
ARTICLE DOI: 10.31480/2330-4871/033
ORIGINAL RESEARCH OPEN ACCESS
Selection of anesthetic agents for caesarean section: A survey of current obstetric anesthesia practice in China
Jeffrey Huang, MD1 , Huan Gao, MD2
1Anesthesiologists of Greater Orlando &University of Central Florida
2Department of Anesthesiology, Fangcheng County Hospital, Henan, China
Jeffrey Huang, MD. Anesthesiologists of Greater Orlando &University of Central Florida, 2699 Lee Rd, Suite 510, Winter Park, FL 32789, Tel: 4078969500, Fax: 4078969585, Email: jeffhuangmd@gmail.com
Editor: Henry Liu, MD, MS, Associate Professor of Anesthesiology Vice Chairman for Scholarly Activities Department of Anesthesiology & Perioperative Medicine Hahnemann University Hospital Drexel University College of Medicine 245 North 15th Street, MS 310 Philadelphia, PA 19102, (215)762-7877 Email: jeffreyhuangmd@gmail.com
Received: November 02, 2015 | Accepted: November 18, 2015 | Published: December 08, 2015
Citation: Huang J. Hao H. Selection of anesthetic agents for caesarean section:A survey of current obstetric anesthesia practice in China. Transl Perioper & Pain Med 2016; 1(1): 32-38
Abstract
Background
A national survey of current obstetric anesthesia practice and anesthetic induction agents for cesarean section was undertaken.
Methods
All registered members of New Youth Anesthesia Forum (a popular anesthesia social network in China) were invited to response to the survey.
Results
A total of 653 responses were received. Propofol was the current routine induction agent of choice for cesarean section used by 70.75% respondents. 92.34% believed that propofol is indicated for induction general anesthesia for cesarean section. 82% would support a change to the use of propofol to replace ketamine as the induction agent of choice for cesarean section. A majority of cesarean section (elective or emergency) were done under regional anesthesia.
Conclusions
This survey suggested that propofol is the most commonly used induction agent in obstetric practice in China. Anesthesiologists strongly supported the use of propofol to replace ketamine as the induction agent of choice for cesarean section, manufacture should change their statement in their package insert about the use of propofol in obstetric anesthesia.
Keywords
propofol, obstetric anesthesia, contraindication, survey
Choice of anesthesia for Cesarean section (CS) must be made by taking into consideration several factors, such as, anesthetic, obstetrical and fetal risk factors. Regional anesthesia is usually preferred because of its advantages of maternal safety. Significant efforts have been made to avoid general anesthesia for Cesarean delivery. General anesthesia is chosen in emergency situations, or when neuraxial anesthesia techniques have failed or are contraindicated [1].
Thiopental has been routinely used as an anesthetic induction agent for cesarean section since the 1930s. Thiopental is no longer available in many western countries. Propofol became the alternative.
In China, thiopental is also not available. Ketamine was recommended as a drug of choice for induction of general anesthesia during cesarean delivery by obstetric anesthesia society [2]. Frequent shortage of ketamine prevented selection of ketamine as an induction agent for obstetric anesthesia. Propofol is specifically contraindicated for obstetric anesthesia by its manufacturer.
We surveyed Chinese anesthesiologists about their drug choices for induction GA for CS and their opinions about the propofol usage during pregnancy.
Methods
There are more than 78,000 registered anesthesiologists members in New Youth Anesthesia Forum. After approval from the committee of New Youth Anesthesia Forum, a survey was sent to all members of anesthesiologists by Wechat. The respondents can choose mobile device or desktop to complete the survey.
The survey (Appendix A) was designed to ask questions about GA for cesarean delivery; especially, the choice of induction agents, and the use of propofol for GA in obstetric settings, their opinions about manufacturers' the statement that "propofol is not licensed for use in obstetric anesthesia".
The survey questions included basic demographic information about the anesthesiologist's hospital level (grade I, II, III), number of delivery per annum, working experience, obstetric anesthesia specialty training.
Statistical analyses were performed using Chi square test. All tests were 2-tailed with a type I error rate of 0.05.
Results
A total of 653 responses were received. Majority of surveys (640) were completed by mobile devices, the rest [13] was received by computer.
Participant's demographic data is presented in Table 1:
Table 1: Demographic data
| Gender | Male: 451 (69%) | Female: 202 (31%) |
|---|---|---|
| OB anesthesia specialty training | Yes: 264 (40%) | No: 389 (60%) |
| Working experience (years) | ||
| 0-5 | 108 (16.54% | |
| 5-10 | 162 (24.81%) | |
| 10-20 | 251 (38.44%) | |
| >20 | 132 (20.21%) | |
| Physician title | ||
| Resident physician | 154 (23.58%) | |
| Attending Physician | 323 (49.46%) | |
| Director Physician | 132 (20.21%) | |
| Physician title | ||
| Resident physician | 154 (23.58%) | |
| Attending Physician | 323 (49.46%) | |
| Director Physician | 176 (26.95% | |
| Hospital level | ||
| Grade I | 21(3.22%) | |
| Grade II | 202 (43.34%) | |
| Grade III | 349 (53.45% | |
| Number of births each year | ||
| < 5000 | 385 (59.96%) | |
| 5000-10000 | 198 (30.32%) | |
| >10000 | 70 (10.72%) |
The responders were distributed in Shanghai 22%, Guangdong 18%, Tianjin 16%, Sichuan 10%, Hubei 6%, Henan 3%, Beijing 2%, Hunan 2%, Shandong 2%, Zhejiang 2%, the rest of country 17%.
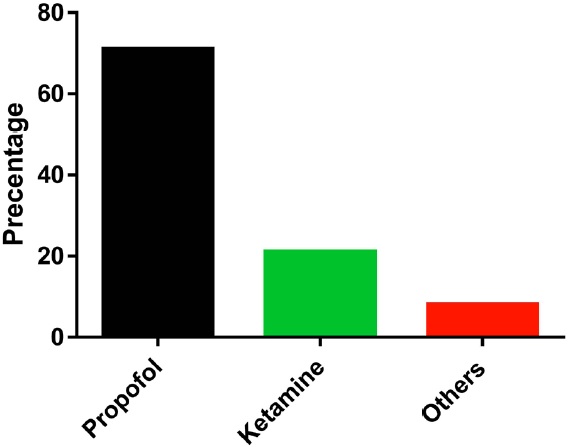
Propofol was the current routine induction agent of choice for cesarean section used by 70.75% respondents, Ketamine was used by 21.13%, and other agents were used by 8.12% (Fig 1).
Figure 1: Percentage of the use of induction agents for obstetric general anesthesia
When participants were asked whether propofol is indicated in a patient undergoing Cesarean section under general anesthesia, 92.34% answered propofol is indicated for the patient undergoing cesarean section, only 7.66% said that propofol is contraindicated for induction GA for CS.
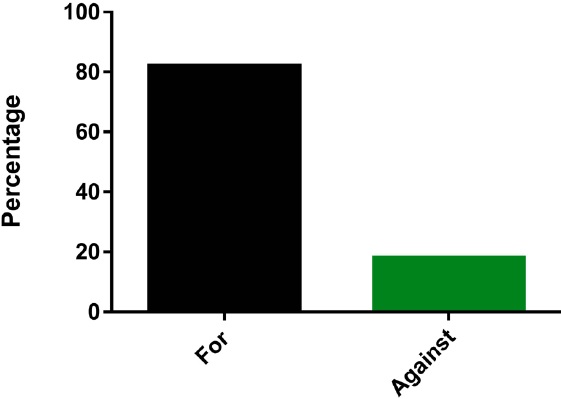
Participants were asked if they would support a change to the use of propofol to replace ketamine as the induction agent of choice for CS. 82% would support such a change. However, 18% would not support.
Participants were asked whether they would support the statement that "propofol is not licensed for use in obstetric anesthesia". 86% respondents answered that manufacture should delete the contraindication statement from the package insert. Only 14% supported manufacture's statement (Fig 2).
Figure 2: Percentage of supporting a change to propofol from ketamine for obstetric general anesthesia
When the respondents were stratified by title, the response about a change to the use of propofol to replace ketamine as the induction agent of choice for CS, there were significant difference between resident physician group and director physicians group (P < 0.05) (Table 2).
Table 2: Number of supporting a change to propofol for obstetric general anesthesia among different physician groups
| Support the use of propofol to replace ketamine | Do not support the use of propofol to replace ketamine | |
|---|---|---|
| Resident Physicians* | 118 | 36 |
| Attending Physicians | 265 | 58 |
| Director Physicians* | 150 | 26 |
*P< 0.05
Most of the practitioners (94%) reported that they performed elective cesarean deliveries under neuraxial anesthesia. A majority of emergency cesarean section were done under regional anesthesia (82%). 17% percentage of emergency cesarean section were performed under general anesthesia compared to 5% elective cesarean section (Table 3).
Table 3: Types of anesthesia provided during CS
| Regional anesthesia | General anesthesia | Others | |
|---|---|---|---|
| Elective CS | 94% | 5% | 1% |
| Emergency CS | 82% | 17% | 1% |
Of the respondents, 86% reported that they used rapid sequence induction and intubation (RSI) technique for cesarean section under general anesthesia. The use of the technique was described as always by 58 %, "often" by 28 %. 14% reported "rarely" used the RSI technique.
Of the respondents, endotracheal tube was used by 84.99% participants, LMA was used by 9.49%, face mask was used by 5.51%, when cesarean section was performed under general anesthesia.
Sevoflurane was used by 64% of respondents for maintenance, followed by isoflurane (4%) and desflurane ( < 1%), respectively. No inhalation agents were used by 31%. Majority of respondents reported that they did not use nitrous oxide (96%) during general anesthesia for cesarean section.
Conflict Interests DisclosureWeChat is a free instant messaging service application for smartphone, and developed by Tencent in China. WeChat has been used in many fields of information service by the media, government, hospital, and enterprises etc. Wechat had more than 600million users. It provides a new tool to conduct survey for anesthesiologists. There are more than 78,000 registered anesthesiologists members in New Youth Anesthesia forum (a popular anesthesia social network). All members can receive the survey invitation by WeChat. However, it is unknown exactly how many members read the invitation.
The primary target of this survey was to obtain the opinion of the use of propofol in obstetric anesthesia and current practice of obstetric anesthesia amongst Chinese anesthesiologists. To the best of our knowledge, it is the first study of this topic in China. Locations of respondents showed that the participants were fairly distributed in China.
Thiopental has been used as an anesthetic induction agent for cesarean section since the 1930s. Thiopental remains the most commonly used induction agent in UK obstetric practice in the recent survey [3]. Thiopental is no longer available in many countries, including the United States and Canada, and it is difficult to obtain in some others [4]. Propofol is now the best alternative [3,4]. Multiple studies had been conducted to compare propofol and thiopental for obstetric GA [5-11]. Several studies show no difference between thiopental and propofol, others report a slight short-term neonatal depression with propofol [3, 4]. The growing evidence supported the use of propofol as a standard induction agent for general anesthesia in caesarean section. In the USA, propofol is the first line induction agent in most large obstetric centers [3].
Ketamine can be safely used for the induction of general anesthesia in patients undergoing cesarean section [12, 12, 14]. Ketamine is also recommended as an alternative to thiopental for induction of general anesthesia in patients undergoing CS. Ketamine, etomidate and propofol were recommended as drugs of choice for induction of general anesthesia during cesarean delivery by Chinese obstetric anesthesia society [2]. They also emphasized that propofol should be used with caution. In this survey, Ketamine was used by only 21.13% respondents as the drug of choice for induction of general anesthesia during cesarean delivery. Ketamine is avoided in hypertensive and preeclamptic pregnancy women. Also, recovery after ketamine may be associated with displeasing dreams and/or deliriums [15]. Anesthesiologists frequently faced shortages of ketamine in China. These factors can limit selection of ketamine as induction agents for obstetric anesthesia.
In UK survey, anesthesiologists were asked if they would support a change to the use of propofol as the induction agent of choice for CS. Near 60% would support such a change [3]. In this study, anesthesiologists were asked if they would support a change to the use of propofol to replace ketamine as the induction agent of choice for CS. 82% would support such a change. There were more senior anesthesiologists (director physicians) than younger physicians (resident physicians) to support such a change. Working experience and knowledge of pharmacology may have contributed the difference.
The combination of intravenous induction agents, neuromuscular blockade and tracheal intubation for CS was first described in 1959[16] and, has achieved a significant safety record. The endotracheal tube placement is to prevent the aspiration of regurgitated stomach contents into the trachea. This technique was used by 85% of the respondents in this survey.
Han et al [17] reported the use of the classic laryngeal mask airway (LMA) for elective caesarean section. They recommended LMA might be a useful alternative to tracheal intubation for Cesarean delivery in a carefully selected patient population of relatively low body mass index (BMI) pregnancy women undergoing elective Cesarean section with at least four hours of fasting [17]. In this survey, laryngeal mask airway (LMA) for caesarean section was used by 9.49% respondents. However, it was unknown whether these cases were elective or emergency, and patients' body habitus.
In the UK survey [3], Sevoflurane was used by 52% of respondents, followed by isoflurane and desflurane, respectively. In our survey, sevoflurane was the most popular inhalation agent during general anesthesia for cesarean section. Nitrous oxide is commonly used inhalational agent during general anesthesia for cesarean section because of its minimal effects on maternal blood pressure and uterine tone [18]. However, our survey demonstrated that majority of the respondents did not use nitrous oxide during general anesthesia for cesarean section. Concerns regarding the environmental effects of nitrous oxide may prohibit the use of nitrous oxide in China.
In this survey, propofol is the most commonly used induction agent in obstetric practice, used by 70.75% respondents. Propofol is specifically contraindicated for obstetric anesthesia by its manufacturer. Therefore the use of propofol in obstetric anesthesia became an off label use, and may pose liability exposure to Chinese anesthesiologists.
The practice of prescribing a drug for a purpose other than that for which it is approved is defined as "off-label" use [19]. Off-label use is very common in medical practice worldwide. In pediatric practice, three-fourths of prescription drugs are used off label [19]. Off-label use is not a violation of the standards of care. One of the major reasons of off-label drug use is the unavailability or absence of licensed, effective and safe therapeutic medications [20]. Frequent shortage of ketamine may be a reason that propofol is widely used in obstetric anesthesia in China. In addition, it is not cost effective for pharmaceutical companies to get drugs reapproved for other uses [21]. Therefore the package insert still stated that propofol is contraindicated for obstetric anesthesia.
There are limitations with this study. The survey response rate was not able to be determined. It was unknown how many members had read the survey invitation. The survey study cannot validate the accuracy and honesty of the response. Therefore prospective study is recommended.
In conclusion: this survey suggested that propofol is the most commonly used induction agent in obstetric practice in China. Regional anesthetic techniques are predominant use in Cesarean section. Anesthesiologists strongly supported the use of propofol to replace ketamine as the induction agent of choice for CS, manufacture should change their statement in their package insert about the use of propofol in obstetric anesthesia.
Conflict Interests Disclosure
The authors have no conflicting interests to disclose.
Disclosure of Funding
None
References
- Sandra Lesage (2014): Cesarean delivery under general anesthesia: Continuing Professional Development Can J Anesth 61:489—503 PMID: 24700402
- Yao S. (2011): Quick guide for obstetrics and Gynecology. Chinese Continuing Medical Education.12: 57-58.
- Murdoch H, Scrutton M, Laxton CH (2013): Choice of anaesthetic agents for caesarean section:A UK survey of current practice Int J Obstet Anesth 22, 31—35 PMID: 23122280.
- Rucklidge M (2013). Up-to-date or out-of- date: does thiopental have a future in obstetric general anaesthesia? Int J Obstet Anesth 22: 175-8. PMID: 23711759.
- Capogna G, Celleno D, Sebastiani M, et al (1991). Propofol and thiopentone for caesarean section revisited: maternal effects and neonatal outcome. Int J Obstet Anesth 1:19—23. PMID:15636791.
- Valtonen M, Kanto J, Rosenberg P (1989). Comparison of propofol and thiopentone for induction of anaesthesia for elective caesarean section. Anaesthesia 44:758—62 PMID:2802124.
- Celleno D, Capogna G, Tomassetti M, Costantino P, Di Feo G, et al. (1989) Neurobehavioural effects of propofol on the neonate following elective caesarean section. Br J Anaesth 62:649—54. PMID: 2787664.
- Yau G, Gin T, Ewart MC, Kotur CF, Leung RK, et al. (1991) Propofol for induction and maintenance of anesthesia at caesarean section. A comparison with thiopentone/enflurane. Anaesthesia 1991; 46:20—3. PMID: 1996746.
- Moore J, Bill KM, Flynn RJ, McKeating KT, Howard PJ.(1989) A comparison between propofol and thiopentone as induction agents in obstetric anaesthesia. Anaesthesia 44:753—7. PMID: 2802123
- Gin T, O'Meara ME, Kan AF, Leung RKW, Tan P, et al. (1993) Plasma catecholamines and neonatal condition after induction of anaesthesia with propofol or thiopentone at caesarean section. Br J Anaesth 70:311—6 PMID:8471376.
- Gin T, Gregory MA, Oh TE. (1990) The haemodynamic effects of propofol and thiopentone for induction of caesarean section. Anaesth Intensive Care 18:175—9 PMID: 2368889.
- Baraka A, Dich-Nielsen J, Holasek J.(1982) Ketamine as induction agent for caesarean section Acta Anaesthesiol Scand. 26(2):139-42 PMID: 7102236.
- Krissel J, Dick WF, Leyser KH, Gervais H, Brockerhoff P, et al.(1994) Thiopentone, thiopentone/ketamine, and ketamine for induc- tion of anaesthesia in caesarean section. Eur J Anaesthesiol. 11(2):115-22 PMID: 8174531.
- Nayar R, Sahajanand H (2009). Does anesthetic induction for cesarean section with a combination of ketamine and thiopentone confer any benefits over thiopentone or ketamine alone? A prospective randomized study. Minerva Anestesiol 75: 185-90. PMID 18946429.
- Marshall BE, Longnecker DE. General anesthetics. In: Handman JG, Limbird LE, eds The pharmacological basis of therapeutics. 9th ed. New York: McGraw-Hill, 1996;307-28
- Hamer Hodges RJ, Bennett JR, Tunstall ME, Knight RF.(1959) General anaesthesia for operative obstetrics. Br J Anaesth 31:152—63. PMID: 13651521.
- Han TH, Brimacombe J, Lee EJ, et al (2001). The laryngeal mask airway is effective (and probably safe) in selected healthy parturients for elective Cesarean section: a prospective study of 1067 cases. Can J Anaesth 48:1117-21. PMID: 11744589.
- Tsen L: Anesthesia for cesarean delivery. In: Chestnut D, Wong C, Tsen L, Ngan Kee w, et al. eds Chustnut's Obstetric Anesthesia 4th ed. Philadelphia: Elsevier Mosby 2009; 521-574
- Gazarian M, Graudins LV, Kelly M, McPhee FR, Ward RL, et al. (2006) Off-label use of medicines: consensus recommendations for evaluating appropriateness. Med J Aust. 185(10):544-548 PMID: 17115966.
- Golocorbin S, Ilickovic I, Mikov M (2015): Reasons for and frequency of Off-label drug use. Med Pregl. 68(1-2):35-40. PMID: 26012242.
- Committee on Drugs, American Academy of Pediatrics (2002). Uses of drugs not described in the package insert. Pediatrics. 110(1 Pt1):181-183. PMID 12093968.