Translational Perioperative and Pain Medicine (ISSN: 2330-4871)
ARTICLE DOI: 10.31480/2330-4871/209
Review Article | Volume 12 | Issue 1 Open Access
Anesthesia-Induced Fatigue Spectrum in Perioperative Care (Part 2): Implementation Pathway and Department-Level Quality Improvement
Qin Yin1#, Ming-Yue Cheng1#, Shu Wang2, Yu-E Sun3, Jin-Feng Wang4* and Wei Cheng5*
1The Affiliated Hospital of Xuzhou Medical University, PR China
2Yancheng Third People's Hospital, Yancheng, PR China
3Drum Tower Hospital Affiliated to Nanjing University Medical College, PR China
4The Suzhou Hospital of the Chinese Academy of Traditional Chinese Medicine - Xiyuan Hospital, PR China
5The Affiliated Huai'an No.1 People's Hospital of Nanjing Medical University, PR China
Wei Cheng, MD, The Affiliated Huai'an No.1 People's Hospital of Nanjing Medical University, Huai'an 223300, China, Tel: +8618796205791;Jin-Feng Wang, MD, The Suzhou Hospital of the Chinese Academy of Traditional Chinese Medicine - Xiyuan Hospital, PR China, Tel: +8618168779112
Editor: Renyu Liu, MD; PhD; Professor, Department of Anesthesiology and Critical Care, Perelman School of Medicine at the University of Pennsylvania, Center of Penn Global Health Scholar, 336 John Morgan building, 3620 Hamilton Walk, Philadelphia, PA 19104, USA, Fax: 2153495078, E-mail: RenYu.Liu@pennmedicine.upenn.edu
Received: Sep 16, 2025 | Accepted: Nov 11, 2025 | Published: Nov 15, 2025
Citation: Qin Yin, Ming-Yue Cheng, Shu Wang, et al. Anesthesia-Induced Fatigue Spectrum in Perioperative Care (Part 2): Implementation Pathway and Department-Level Quality Improvement. Transl Perioper Pain Med 2025;12(2):777-787
Abstract
Part 1 defined the Anesthesia-Induced Fatigue Spectrum (AIFS) as classifiable, quantifiable, and actionable fatigue phenotypes arising when anesthesia-related exposures interact with four axes-inflammation/metabolism, neural circuits/arousal, circadian/sleep, and mood/cognition. It specified standardized assessment windows (baseline ≤ 7 days pre-op; POD 1/3/7/30; optional POD 90) and recommended parallel readouts with PROMIS®-Fatigue (T-scores) and Quality of Recovery-15 (QoR-15), complemented by digital phenotypes (steps/activity intensity, nocturnal sleep efficiency/arousals, and heart-rate variability).
Building on that foundation, Part 2 is a methods-first, practice-oriented paper that operationalizes AIFS for routine quality improvement. We outline ERAS-compatible bundles (risk-stratified antiemesis; opioid-sparing within multimodal analgesia; circadian-friendly conduct of anesthesia), ward workflows and nurse checklists, and a minimal EHR/ward-dashboard field map to capture the prespecified windows with a single set of parallel readouts. We provide reporting templates (endpoint hierarchy, estimation-first summaries with 95% CIs, and responder analyses using the QoR-15 MCID ≈ 6 points) and governance safeguards for digital streams (completeness checks, false-alert control, privacy/security and equity-by-design), with pragmatic feasibility notes on adherence targets and site-tailored data pipelines.
This framework emphasizes estimation over hypothesis chasing, prioritizes transportable documentation over bespoke analytics, and does not present new validation datasets or predictive models. Overall, AIFS Part 2 enables quantifiable fatigue tracking and continuous improvement across perioperative pathways.
Keywords
Anesthesia-Induced fatigue spectrum, Fatigue-Centered anesthesia quality indicators, AIFS-Bundle (Anesthesia-Induced Fatigue Spectrum Bundle), ERAS, PROMIS®-Fatigue
Introduction - Rationale and Objectives
Whether the Anesthesia-Induced Fatigue Spectrum (AIFS) can be integrated into Enhanced Recovery After Surgery (ERAS) hinges on two points: shared objectives and interoperable implementation units. ERAS is organized around the sequence “mitigate surgical stress-maintain organ function-promote recovery,” with patient-centered workflows and audit as core tenets. AIFS elevates the “fatigue burden” from a secondary outcome to a core endpoint and calls for serial, comparable measurements at key decision nodes-anesthetic induction, maintenance, emergence, and approximately 72 hours postoperatively-so that interventions can be adjusted accordingly. The two frameworks share a “common language” of standardized endpoints and process indicators: for subjective recovery, PROMIS®-Fatigue and Quality of Recovery-15 (QoR-15); for processes, opioid-sparing with regional multimodal analgesia, risk-stratified multimodal antiemesis with protocolized rescue-class switching, and, when appropriate, a preference for total intravenous anesthesia (TIVA) to reduce postoperative nausea and vomiting (PONV)-all practices that align with ERAS and are easy to embed [1-3]. In other words, AIFS does not rebuild the house; it incorporates a frequently overlooked yet experience-critical dimension-fatigue-into the existing ERAS governance framework: Endpoints are measurable, pathways are auditable, and effects are comparable, often without additional resources across procedures or institutions. Consequently, AIFS can function both as ERAS’s depth dimension (targeting fatigue–sleep–affect–autonomic domains) and as an anesthesia quality lever that works in concert with nutrition, fluid management, and early mobilization [1-3].
Roadmap
The manuscript follows an IMRaD-like flow-Introduction → Endpoints/Windows → Framework (axes & F-AQI) → AIFS-Bundle → Conclusion-so that methodological choices and reporting guidance are easy to locate.
Scope note
This Part 2 is a pragmatic, methods‑first paper focused on ward workflow, EHR hooks, and reporting templates under the AIFS windows; it does not include new validation datasets, procedure‑stratified meta‑analysis, or predictive modelling. This framework enables quantifiable fatigue tracking and continuous improvement across perioperative pathways.
Reference note
Key sources were verified for currency and diversity (2018-2025), with NLM abbreviations and DOIs standardized.
Bringing postoperative fatigue under quality governance requires converting patient complaints into stable, trackable endpoints. We recommend PROMIS-Fatigue (Patient-Reported Outcomes Measurement Information System-Fatigue) as the primary fatigue endpoint, with scoring and follow-up conducted per the official manual; in parallel, use QoR-15 to characterize early recovery and interpret change with published MCID (minimal clinically important difference) and population validation data. To couple process and outcome, include composite measures such as DAH30 (Days Alive and at Home at 30 days), which synthesize length of stay, readmission, and discharge destination into a single recovery trajectory signal. This endpoint set aligns with the terminology and reporting framework of StEP (Standardised Endpoints in Perioperative Medicine)/COMPAC (Core Outcome Measures in Perioperative and Anaesthetic Care), facilitating cross-service audit and internal/external benchmarking [4-10].
Parallel Capture of Digital Phenotypes in AIFS-Steps, Sleep Efficiency, and HRV to Objectify the “Fatigue Trajectory”
Synchronizing wearable data with perioperative decision nodes yields a continuous recovery curve and helps identify patients deviating from the expected course in real time [11-12].
Activity
Daily step counts and activity intensity reflect the pace of functional recovery; lower postoperative steps have been associated with higher risks of complications or unplanned readmission [13-14].
Sleep
Sleep efficiency and an awakening index provide a window on nocturnal restoration; among older adults, poor subjective sleep on the first postoperative night is independently associated with delirium [15].
Autonomic tone
Heart-rate variability (HRV) characterizes autonomic load and circadian re-entrainment; compared with single time points, multi-epoch or dynamic monitoring has greater interpretive value for risk stratification and early warning [16].
At the department level, running these digital indicators in parallel with patient-reported scales converts the “fatigue trajectory” into auditable, reviewable process signals for routine governance and feedback [11-16]
Overview of the Six-Cluster AIFS Framework-A “Mechanism-Phenotype-Intervention” Traffic Map
The Anesthesia-Induced Fatigue Spectrum (AIFS) organizes anesthesia-related fatigue into six clusters. For each cluster it defines measurable indicators, matched interventions, and readout windows, allowing alignment with Enhanced Recovery After Surgery (ERAS) workflows and node-based audit/benchmarking. Prior studies have linked ERAS adherence to improved outcomes, which supports this governance-oriented design [17] (Figure 1).
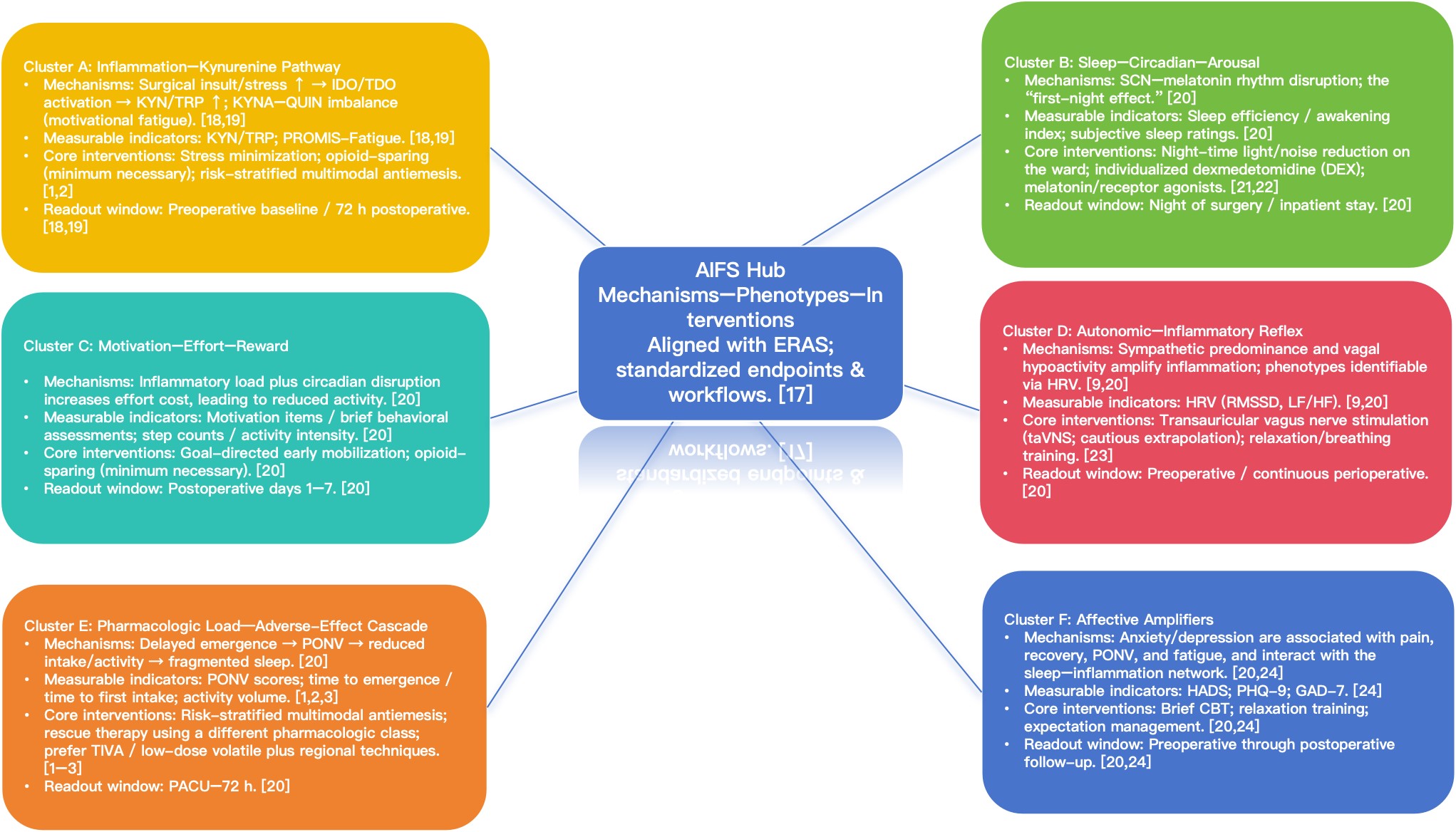
Figure 1:
Overview of the AIFS Six-Cluster Framework -“Mechanisms-Phenotypes-Interventions” Traffic Map.AIFS organizes anesthesia-related fatigue mechanisms into six clusters and, for each cluster, specifies “measurable indicators-matched interventions-readout windows,”enabling alignment with ERAS workflows and node-wise audit/benchmarking; prior studies indicate an association between ERAS adherence and outcomes.
Abbreviations: 5-HT3: 5-Hydroxytryptamine 3 (serotonin) receptor; AI: Arousal Index; AIFS: Anesthesia-Induced Fatigue Spectrum; CAT: Computerized Adaptive Testing; CI (CIs): Confidence interval(s); DAH30: Days Alive and at Home at 30 days; DEX: Dexmedetomidine; e-PRO: Electronic Patient-Reported Outcome(s); ERAS: Enhanced Recovery After Surgery; F-AQI: Fatigue-Centered Anesthesia Quality Indicators; GAD-7: Generalized Anxiety Disorder-7; HADS: Hospital Anxiety and Depression Scale; HF: High-Frequency band; HL7 FHIR: Health Level Seven - Fast Healthcare Interoperability Resources; HRV: Heart Rate Variability; MCID: Minimal Clinically Important Difference; NK1: Neurokinin-1 (receptor); ONC-ISA: Office of the National Coordinator - Interoperability Standards Advisory; PCO IG: Patient-Centered Outcomes Implementation Guide; PDSA: Plan-Do-Study-Act; PHQ-9: Patient Health Questionnaire-9; PONV: Postoperative Nausea/Vomiting; PRO: Patient-Reported Outcome(s); PROMIS: Patient-Reported Outcomes Measurement Information System; PROMIS-Fatigue: Patient-Reported Outcomes Measurement Information System - Fatigue; QoR-15: Quality of Recovery-15; RMSSD: Root-Mean-Square of Successive Differences; SEI: Sleep Efficiency; SOP (SOPs): Standard Operating Procedure(s); TIVA: Total Intravenous Anesthesia
Intervention note
Within Part 2, taVNS, dexmedetomidine for first-night sleep, and melatonin are treated as exploratory, context-dependent options; the core AIFS-Bundle remains risk-stratified antiemesis, an appropriate maintenance technique (including TIVA when suitable), and opioid-sparing within multimodal analgesia.
AIFS-cluster A: Inflammation-kynurenine pathway
Surgical injury or stress can upregulate indoleamine 2,3-dioxygenase (IDO) and tryptophan 2,3-dioxygenase (TDO), shifting tryptophan metabolism toward the kynurenine branch; an elevated kynurenine/tryptophan (KYN/TRP) ratio signals activation of the inflammation–metabolism axis. Imbalance between kynurenic acid (KYNA) and quinolinic acid (QUIN) relates to motivation/reward circuitry, and patients may present with a “want to act but cannot” motivational fatigue phenotype [18-19]. Clinically, a sensible base includes stress-reduction measures, opioid-sparing (minimum necessary), and risk-stratified multimodal antiemesis; in higher-risk patients, concurrent monitoring of KYN/TRP together with fatigue scales can be considered.
AIFS-cluster B: Sleep-circadian-arousal network and the “First-Night Effect”
Anesthesia and ward conditions can disrupt the suprachiasmatic nucleus (SCN)-melatonin rhythm and precipitate a first-night effect, which is associated with poorer subjective recovery and a higher risk of certain complications [20]. In selected patients and at appropriate dosing times, dexmedetomidine (DEX) may improve subjective sleep and elements of sleep architecture, but it should be individualized with vigilance for bradycardia and hypotension. Melatonin or melatonin-receptor agonists may be beneficial when dose and timing are well matched, acknowledging heterogeneity in response [21,22]. At the ward level, prioritize night-time light and noise reduction and minimize nonessential nocturnal interventions to provide a stable substrate on which pharmacologic strategies can act [20].
AIFS-cluster C: Neural circuits/arousal & motivational fatigue
Motivational fatigue reflects altered effort-reward appraisal and reduced willingness to initiate or sustain goal-directed activity, which we conceptualize as an arousal-valuation phenotype within AIFS [1,3].
Experimental and clinical observations link this phenotype to the tryptophan-kynurenine pathway-particularly shifts in KYNA/QUIN balance-implicating cortical-striatal excitation/inhibition and motivational drive [7].
Under wake pressure and energetic stress, adenosine accumulation engages A1/A2A receptors, reducing cortical excitability and biasing the effort–arousal balance toward “low-activation/low-persistence” states [8].
In perioperative contexts, analgesia, antiemesis, sleep/circadian care, and opioid-sparing strategies can indirectly improve motivational fatigue by lowering sickness-behaviour load and facilitating early activity, rather than by a single “arousal drug” effect [1,4,5].
Accordingly, AIFS operationalizes this cluster with parallel readouts-PROMIS-Fatigue (T-scores) for perceived energy, QoR-15 for global comfort/recovery, and digital phenotypes (steps/activity intensity; nocturnal SEI/AI) to quantify goal-directed behaviour in standardized windows (baseline ≤ 7 d; POD 1/3/7/30; optional POD 90) [1,3,4].
To avoid over-interpretation across procedures/devices, we recommend estimation-first reporting with prespecified rules and sensitivity analyses, rather than universal thresholds, for activity/sleep metrics in this cluster [11,15].
Clinically, the actionable target is “effort cost” reduction-antiemetic prophylaxis with rescue, multimodal/individualized opioid-sparing, circadian-friendly nursing, and expectation-setting-to lower the barrier to early mobilization and participation in care pathways [1,4,16,17].
Intervention note
Within Part 2, taVNS, dexmedetomidine for first-night sleep, and melatonin are treated as exploratory, context-dependent options; the core AIFS-Bundle remains risk-stratified antiemesis, an appropriate maintenance technique (including TIVA when suitable), and opioid-sparing within multimodal analgesia. (see §5-§6 for details).
AIFS-cluster D: Mood/cognition & vagus-mediated modulation
Preoperative anxiety/depression is associated with worse early recovery and may amplify pain and sleep disruption, thereby worsening fatigue phenotypes within AIFS [12].
The “inflammatory reflex” provides a mechanistic rationale that vagus-mediated cholinergic signalling can restrain peripheral inflammation and potentially lower central inflammatory load, but translational certainty is limited [9].
Human studies of vagus-nerve-based approaches (including transcutaneous auricular VNS) remain small and heterogeneous, with anxiety/sleep outcomes more commonly reported than fatigue per se and with variability in timing, dose, and endpoints [20,23].
Given these constraints, routine clinical use of VNS/taVNS for postoperative fatigue is not currently supported; if considered, it should occur under preregistered protocols aligned to AIFS windows with parallel readouts (PROMIS-Fatigue, QoR-15, digital phenotypes) and explicit safety monitoring [1,3,9].
For routine care, AIFS emphasizes a screen → educate → targeted support sequence-brief anxiety screening, expectation management, circadian-friendly nursing, and multimodal analgesia/antiemesis-to address mood-linked amplifiers without over-promising device effects [1,3,12].
Reporting should use estimation with confidence intervals, prespecified covariates (pain/sleep/mood), and data-completeness metrics to ensure interpretability and comparability across sites and procedures [1,3].
AIFS-cluster E: Pharmacologic load-adverse-effect cascade
A cascade of delayed emergence → postoperative nausea and vomiting (PONV) → restricted intake/activity → fragmented nocturnal sleep magnifies fatigue and slows recovery. [20] Baseline management centers on risk-stratified, multimodal antiemesis, and when rescue is needed, switch to an agent from a different pharmacologic class to avoid repeat-exposure chains [1,2]. Where resources and indications permit, prefer total intravenous anesthesia (TIVA) or low-dose volatile in combination with regional analgesia and opioid-sparing; this approach can reduce PONV and improve selected recovery metrics. Evidence for the impact of “residual sedation” is mixed and should be interpreted in the context of patient population and anesthetic regimen [1-3].
AIFS-cluster F: Affective amplifiers
Preoperative anxiety/depression correlates with several adverse postoperative outcomes (e.g., pain and recovery quality); some studies also suggest higher PONV and greater fatigue burden, with bidirectional interactions across the sleep-inflammation network-making this a priority domain for perioperative management [20,24]. Practical steps include rapid screening with Hospital Anxiety and Depression Scale (HADS), Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7); for positives, consider brief cognitive-behavioral strategies, relaxation training, and expectation management, implemented in parallel with antiemesis, analgesia, and circadian-friendly measures to dampen the affect–symptom positive feedback loop. The intensity and timing of interventions should be tailored to patient characteristics and team resources [20,24].
F-AQI (Fatigue-Centered Anesthesia Quality Indicators)
Scope note. In this manuscript, the core AIFS bundle prioritizes risk-stratified antiemesis, an appropriate maintenance technique (including TIVA when suitable), and opioid-sparing within multimodal analgesia; taVNS, dexmedetomidine for first-night sleep, and melatonin are considered exploratory and context-dependent [15,17,19,20] (Figure 2).
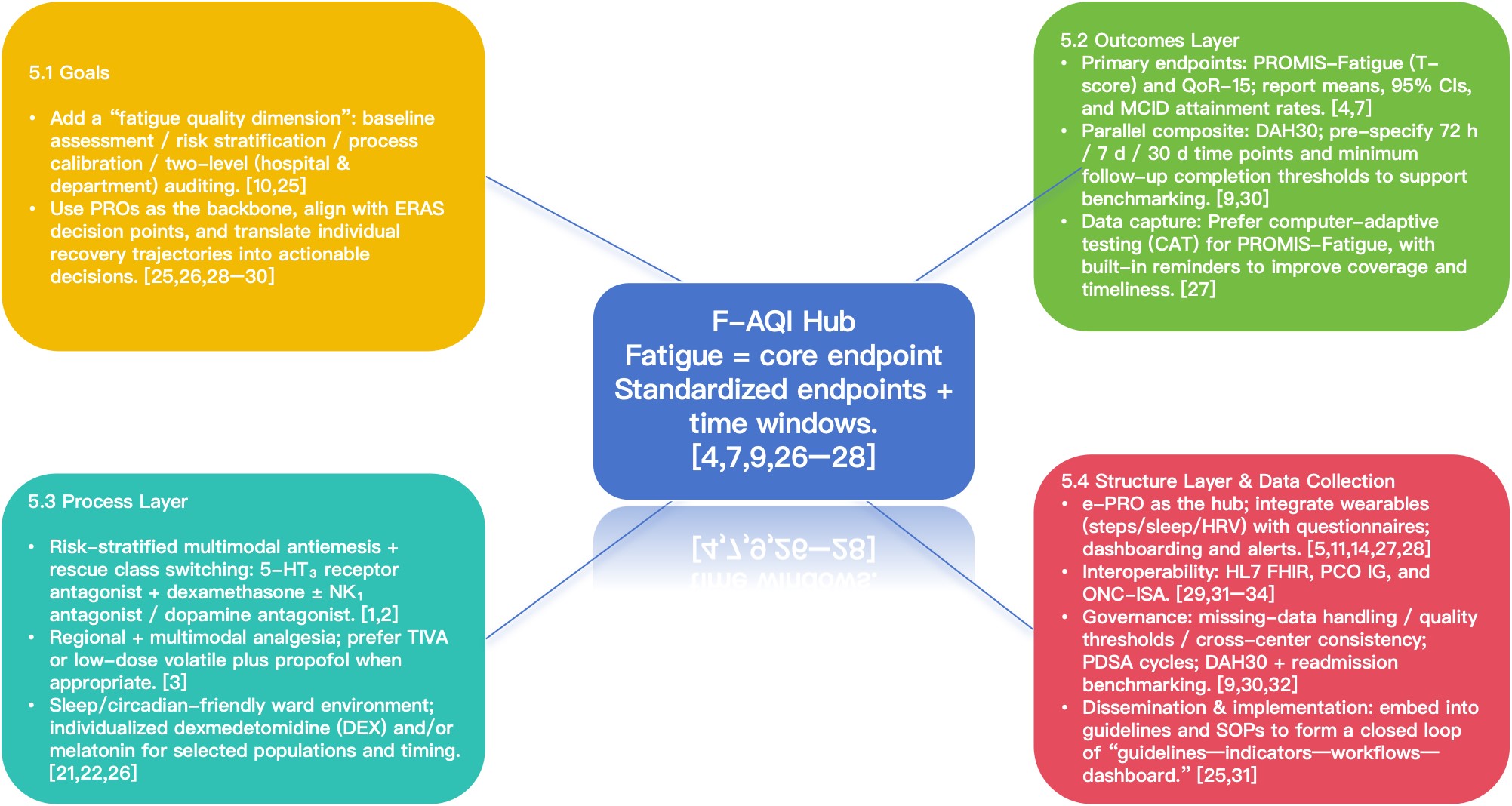
Figure 2:
F-AQI (Fatigue-Centered Anesthesia Quality Indicators).Objectives: Incorporate the measurability, comparability, and modifiability of the “fatigue burden” into the anesthesia quality framework; treat patient-reported fatigue and functional recovery as co-primary endpoints; use standardized endpoints and time windows as the operational levers.
Design: Anchor on endpoints (PROMIS-Fatigue, QoR-15, DAH30) and predefined follow-up windows; aim for executable workflows; build a reusable data backbone to support benchmarking across procedures and institutions.
Abbreviations: 5-HT3: 5-Hydroxytryptamine 3 (serotonin) receptor; AI: Arousal Index; AIFS: Anesthesia-Induced Fatigue Spectrum; CAT: Computerized Adaptive Testing; CI (CIs): Confidence interval(s); DAH30: Days Alive and at Home at 30 days; DEX: Dexmedetomidine; e-PRO: Electronic Patient-Reported Outcome(s); ERAS: Enhanced Recovery After Surgery; F-AQI: Fatigue-Centered Anesthesia Quality Indicators; GAD-7: Generalized Anxiety Disorder-7; HADS: Hospital Anxiety and Depression Scale; HF: High-Frequency band; HL7 FHIR: Health Level Seven - Fast Healthcare Interoperability Resources; HRV: Heart Rate Variability; MCID: Minimal Clinically Important Difference; NK1: Neurokinin-1 (receptor); ONC-ISA: Office of the National Coordinator - Interoperability Standards Advisory; PCO IG: Patient-Centered Outcomes Implementation Guide; PDSA: Plan-Do-Study-Act; PHQ-9: Patient Health Questionnaire-9; PONV: Postoperative Nausea/Vomiting; PRO: Patient-Reported Outcome(s); PROMIS: Patient-Reported Outcomes Measurement Information System; PROMIS-Fatigue: Patient-Reported Outcomes Measurement Information System - Fatigue; QoR-15: Quality of Recovery-15; RMSSD: Root-Mean-Square of Successive Differences; SEI: Sleep Efficiency; SOP (SOPs): Standard Operating Procedure(s); TIVA: Total Intravenous Anesthesia
F-AQI brings the measurability, comparability, and modifiability of the perioperative “fatigue burden” into the anesthesia quality framework. Beyond traditional safety and complication metrics, patient-reported fatigue and functional recovery are elevated as co-primary endpoints, with standardized endpoints and time windows used as the practical levers for implementation [4,9,10,25].
The design centers on clearly specified endpoints-PROMIS-Fatigue (Patient-Reported Outcomes Measurement Information System-Fatigue), QoR-15, and DAH30 (Days Alive and at Home at 30 days)-and predefined follow-up windows; workflows are shaped for executability, and a reusable data backbone is built so results are comparable and transferable across procedures and institutions [4,7,9,26-28].
Goals of F-AQI
Within existing complication and process-quality systems, add a fatigue quality dimension to support preoperative baseline assessment, perioperative risk stratification, process calibration, and two-level (hospital and department) audit-so that relevant information can be tracked and reviewed [10,25]. This dimension anchors on patient-reported outcomes (PROs), aligns with key ERAS (Enhanced Recovery After Surgery) decision points, and converts individual recovery trajectories and aggregate performance into actionable guidance for clinical decision-making [25,26,28-30].
Outcomes layer of F-AQI
Use PROMIS-Fatigue (Patient-Reported Outcomes Measurement Information System-Fatigue) T-scores and QoR-15 as the primary endpoints. Report means, 95% confidence intervals (CI), and minimal clinically important difference (MCID) attainment rates, and display individual fatigue trajectories with rapid vs. delayed recovery subgroups to aid interpretation and stratification [4,7].
To strengthen interpretability for function and resource use, run DAH30 (Days Alive and at Home at 30 days) in parallel. Predefine and make public the key assessment time points (e.g., postoperative 72 h, 7 d, 30 d) and the minimum follow-up completion thresholds to support cross-center benchmarking and hierarchical analyses [9,30].
To reduce measurement burden without sacrificing precision, prioritize computerized adaptive testing (CAT) for PROMIS-Fatigue and embed automated triggers/reminders into ward workflows [27].
Process layer of F-AQI
Focus on three modifiable domains
(1) Risk-stratified antiemesis with predefined rescue: Implement combination prophylaxis according to risk scores (a 5-HT3 receptor antagonist + dexamethasone ± NK1 antagonist/dopamine antagonist). When rescue is required, switch to a pharmacologic class different from prophylaxis to reduce PONV and repeated exposure chains [1,2].
(2) Regional + multimodal analgesia with opioid-sparing: Where resources and indications permit, prefer TIVA (total intravenous anesthesia)-or low-dose volatile plus propofol-to lower PONV and improve selected recovery metrics. Evidence regarding “residual somnolence/sedation” is mixed; interpret in the context of the target population and anesthetic regimen [3].
(3) Sleep/circadian-friendly ward practices: Reduce nocturnal light and noise and minimize nonessential nighttime interruptions. For selected populations and time windows, consider short-course, individualized dexmedetomidine (DEX) or melatonin/receptor agonists, with appropriate monitoring and risk-benefit balancing [21,22,26].
Structure layer and data capture (F-AQI)
(1) Data hub: Use electronic patient-reported outcomes (e-PRO) as the system backbone; prioritize PROMIS-Fatigue collection via computerized adaptive testing (CAT) with built-in reminders. Integrate wearable streams-steps/activity intensity, sleep efficiency/awakening index, heart-rate variability (HRV)-with questionnaires under a unified data dictionary and interface, and expose dashboard-based displays and alerts [5,11,14,27,28].
(2) Interoperability: Adhere to HL7 FHIR (Health Level Seven-Fast Healthcare Interoperability Resources) and its Patient-Centered Outcomes Implementation Guide (PCO IG); reference ONC-ISA (Office of the National Coordinator-Interoperability Standards Advisory) to reduce integration cost and enhance external verifiability [29,31,34].
(3) Governance and improvement: Pre-specify missing-data handling, quality-control thresholds, and cross-center consistency checks. Combine DAH30 with readmission data for “soft–hard” benchmarking, and embed key indicators in PDSA (Plan–Do–Study–Act) cycles to drive continuous improvement and evidence accumulation [9,30,32].
(4) Dissemination and implementation: Co-integrate ERAS pathway updates and F-AQI indicators into specialty guidelines and departmental SOPs (standard operating procedures) to form a closed loop of “guidelines-indicators-workflows-dashboard” [25,31].
Integrated PNEF/AFP2 Model and the Anti-Fatigue Anesthesia Bundle (AIFS-Bundle)
Status. Interventions discussed in this section (e.g., dexmedetomidine for first-night sleep, melatonin) are exploratory, context-dependent, and secondary to the core bundle prioritized in §5.
The PNEF/AFP2 framework connects mechanisms → phenotypes → care pathways for fatigue management: Peripheral inflammatory-metabolic changes (P) signal through the kynurenine pathway and cytokines to Neural circuits (N), with bidirectional crosstalk to Endocrine/Circadian systems (E) and the Fascia-Autonomic-somatic network (F). AFP2 (Anti-Fatigue Phenotype-to-Pathway) then closes the loop by translating pathway → phenotype → pathway-of-care, allowing phenotype-anchored interventions to be deployed at defined time windows. For hospital-level audit and benchmarking, we recommend mapping these mechanisms and phenotypes to dashboarded short-term outcomes and process indicators, and specifying-by risk tier-the minimum follow-up completion rates and missing-data rules needed to support continuous improvement driven by Plan-Do-Study-Act (PDSA) cycles [35,36] (Figure 3).
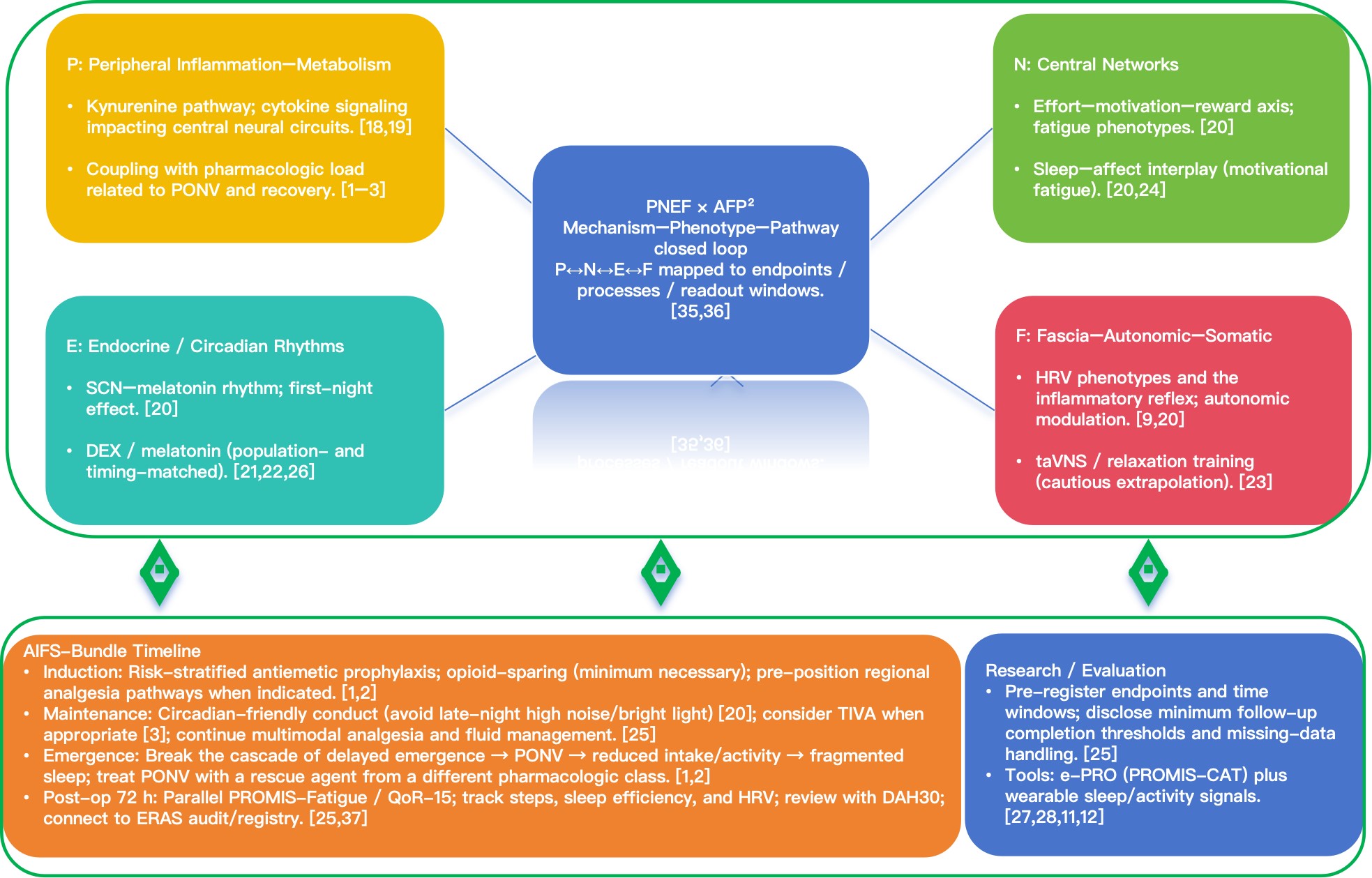
Figure 3:
Integrated PNEF/AFP2 Model and the Anti-Fatigue Anesthesia Bundle (AIFS-Bundle).PNEF/AFP2 links fatigue management across “mechanisms-phenotypes-pathways”: P (peripheral inflammation-metabolism) → N (central neural circuits), interacting with E (endocrine/circadian rhythms) and F (fascia-autonomic-somatic network); AFP² closes the loop from pathways → phenotypes → care pathways, and maps these to dashboarded endpoints and process indicators for audit and benchmarking.
Abbreviations: AIFS-Bundle: Anti-Fatigue Anesthesia Bundle; AFP2: Anti-Fatigue Phenotype-to-Pathway; PACU: Post-Anesthesia Care Unit; PNEF: Peripheral-Neural-Endocrine-Fascia (fascia-autonomic-somatic network); StEP: Standardized Endpoints in Perioperative Medicine
AIFS-T: A technique gradient tiered by fatigue risk
Select combinations that lower pharmacologic load and minimize circadian disruption without adding perioperative complexity:
(1) Preferred strategy. Build on regional analgesia plus multimodal analgesia; apply risk-stratified multimodal antiemesis (a 5-HT₃ receptor antagonist + dexamethasone ± NK₁ antagonist/dopamine antagonist), and use rescue therapy from a different pharmacologic class. Where resources and indications allow, prefer total intravenous anesthesia (TIVA) to reduce postoperative nausea and vomiting (PONV) and steady early recovery [1,2].
(2) Supportive measures. Maintain a sleep/circadian-friendly perioperative environment-reduce night-time light and noise and minimize nonessential nocturnal interventions-to avoid worsening the first-night effect [20].
(3) Special circumstances. Combinations of high-dose opioids + high-concentration volatile agents without antiemetic or sleep-support strategies should be used only short-term when compelled by contraindications or resource limits, with predefined exit criteria and risk controls in place [1,2,20].
AIFS × ERAS: The AIFS-Bundle
Packaged deployment at four decision nodes-induction, maintenance, emergence, and 72 h postoperatively.
Along the timeline:
(a) Induction Implement risk-stratified antiemetic prophylaxis; adopt an opioid-sparing (minimum-necessary) strategy; pre-position regional analgesia pathways when indicated [1,2].
Intervention note Within Part 2, taVNS, dexmedetomidine for first-night sleep, and melatonin are treated as exploratory, context-dependent options; the core AIFS bundle remains risk-stratified antiemesis, an appropriate maintenance technique (including TIVA when suitable), and opioid-sparing within multimodal analgesia. Statistical scope note Part 2 provides reporting guidance (estimation, MCID, CI, trajectories) and does not present primary patient-level analyses.(b) Maintenance. Keep circadian-friendly conduct of anesthesia-avoid late-night high noise and bright light stimulus [20]. Consider total intravenous anesthesia (TIVA) when indications and resources permit [2]. Continue multimodal analgesia and goal-directed fluid management [25].
(c) Emergence. Actively break the cascade of delayed emergence → postoperative nausea and vomiting (PONV) → restricted intake/activity → fragmented sleep; when rescue is needed, switch to an antiemetic from a different pharmacologic class [1,2].
(d) 72 h postoperative. Run PROMIS-Fatigue and QoR-15 in parallel, supplemented with digital phenotypes (steps, sleep efficiency, heart-rate variability [HRV]); review progress against composite outcomes such as DAH30 (Days Alive and at Home at 30 days). For multi-site rollout, link to national or institutional ERAS registries for benchmarking to track adherence and sustained outcome improvement and to support external validity [25,37].
Research and evaluation essentials
(a) Standardize endpoints and time windows. Pre-register postoperative day (POD) 72 h / 7 d / 30 d assessments and specify minimum follow-up completion thresholds; make the missing-data handling plan publicly available [25].
(b) Tools and feasibility. Use a lightweight workflow that combines electronic patient-reported outcomes (e-PRO)-prioritizing PROMIS-Fatigue via computerized adaptive testing (CAT)-with wearable sleep/activity signals. Evaluate feasibility, adherence, and cost-effectiveness, and ensure operational linkage with workflows that embed wearable monitoring [27,28,11,12].
Implementation Essentials for the AIFS-Bundle
(1) Personnel and governance structure. Led by the anesthesia department, with coordinated input from nursing, ward teams, rehabilitation, and informatics. Designate a project lead and a quality-control liaison to form an integrated clinical–informatics–management unit. Include endpoints–processes–composite outcomes in a two-tier audit (hospital and department) [9,10].
(2) Workflow and dashboards. Encode PROMIS-Fatigue, QoR-15, DAH30, and process metrics-risk-stratified antiemesis, regional + multimodal analgesia, and opioid-sparing (minimum necessary)-into standard operating procedures (SOPs). Use dashboards to display stratified cohorts, adherence, and exception alerts, supporting daily reviews and weekly closure loops [7,9,10].
Tiered rollout (resource-aware) To accommodate resource constraints, we specify a two-stage pathway: Core-an e-PRO platform with QoR-15 at the standard windows (baseline ≤ 7 days pre-op; POD 1/3/7/30; optional POD 90), embedded in ward workflow and dashboards; Enhanced-addition of ward wearables for steps/activity and overnight sleep efficiency/arousal index, with optional HRV (RMSSD/HF) when staffing, budget, and pipelines permit. Both tiers share the same endpoint hierarchy and reporting template (interval-estimate focus; QoR-15 MCID ≈6 points responder analyses), enabling cross-site comparability while controlling cost and workload [7,9,10]. In resource-limited settings, prioritize e-PRO with QoR-15 first; add wearables and HRV only when staffing, devices, and governance capacity are in place.
(3) Data and interoperability. Standardize the data dictionary and interfaces; prioritize electronic patient-reported outcomes (e-PRO) with automated reminders. Implement standardized capture and exchange of questionnaires, responses, scoring, and metadata using FHIR (Fast Healthcare Interoperability Resources) profiles for patient-reported outcomes; enforce permissions and missing-data handling per institutional policy to ensure cross-center benchmarking validity and reusability [7,9,10,33,34].
Reporting note
For effect-size presentation in early pilots, report estimate-with-CI summaries; pooled NNT/NNH require harmonized responder thresholds and dose/route strata and are therefore deferred to future harmonized datasets.
Cost note (pilot before scale-up)
Ahead of wider deployment, we recommend a small time-driven activity-based costing (TDABC) pilot to quantify per-patient staff time, device/licensing and cleaning/replacement costs, and to inform workflow redesign; full CEA and budget-impact modeling are outside the scope of this framework.
Conclusion
Conclusion
The Anesthesia-Induced Fatigue Spectrum (AIFS) reframes fatigue from a secondary outcome into a governable core dimension through a mechanism-phenotype-pathway approach. Under F-AQI and the AIFS-Bundle, using PROMIS-Fatigue, QoR-15, and DAH30 as endpoints and pre-specifying windows at 72 h / 7 d / 30 d converts individual recovery trajectories into auditable process signals [4,7,9,10,25]. At the implementation level, adhere to opioid-sparing (minimum necessary), regional plus multimodal analgesia, and risk-stratified antiemesis with predefined rescue; when indicated and feasible, prefer total intravenous anesthesia (TIVA) to reduce postoperative nausea and vomiting (PONV) and stabilize early recovery [1,2,3]. At the data/structure level, link electronic patient-reported outcomes (e-PRO; prioritize CAT) with wearable signals (steps, sleep efficiency, heart-rate variability [HRV]); implement structured capture and write-back in line with HL7 FHIR / PCO IG / ONC-ISA, and embed indicators within PDSA cycles and multi-center benchmarking to drive continuous improvement and external verifiability [11,14,29-31,33,34].
External-validation note
To ensure generalizability beyond our Chinese multicenter context, we explicitly call for external validation of AIFS readouts-including DAH30 where adopted-across sites operating in diverse health-care economies and delivery models; this will benchmark transportability and inform context-specific adaptation.
Embedding AIFS within ERAS represents a new perioperative quality dimension-transforming fatigue from a subjective complaint into a continuous, auditable performance metric.
Funding
National Natural Science Foundation of China (Project Approval Number: 81200858); Jiangsu Province 333 High-level Talent Training Project [Certificate No.: (2022) No. 3-10-007].
Clinical Trials from Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University,the Huai'an Matching Assistance Special Project (2024-2025).
Conflict of Interest
None.
AI Assisted Declaration
The authors used generative AI tools (e.g., ChatGPT, OpenAI) to assist in language polishing and formatting. All intellectual content, analyses, and conclusions are solely those of the authors.”
Presentation
None Declared.
References
- Weibel S, Schaefer MS, Raj D, Rücker G, Pace NL, et al. (2021) Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: An abridged cochrane network meta-analysis. Anaesthesia 76: 962-973.
- Gan TJ, Belani KG, Bergese SD, Chung F, Diemunsch P, et al. (2020) Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg 131: 411-448.
- Daccache N, Wu Y, Jeffries SD, Zako J, Harutyunyan R, et al. (2025) Safety and recovery profile of patients after inhalational anaesthesia versus target-controlled or manual total intravenous anaesthesia: A systematic review and meta-analysis of randomised controlled trials. Br J Anaesth 134: 1474-1485.
- Rothrock NE, Amtmann D, Cook KF (2020) Development and validation of an interpretive guide for PROMIS scores. J Patient Rep Outcomes 4: 16.
- (2023) User Manual and Scoring Instructions- PROMIS Fatigue. HealthMeasures.
- Myles PS, Myles DB, Galagher W, Chew C, MacDonald N, et al. (2016) Minimal clinically important difference for three Quality of Recovery scales. Anesthesiology 125: 39-45.
- Myles PS, Myles DB (2021) An updated minimal clinically important difference for the QoR-15 scale. Anesthesiology 135: 934-935.
- Le Bescond V, Petit-Phan J, Campfort M, Nicolleau C, Conté M, et al. (2024) Validation of the postoperative QoR-15 questionnaire after emergency surgery and association with quality of life at three months. Can J Anaesth 71: 590-599.
- Ribeiro T, Padley JR, White L (2024) Days at home after surgery as a perioperative outcome: A narrative review. BJA Open 3: 100305.
- Myles PS, Ashbury TL, Boney O (2025) Updated standardised endpoints in perioperative medicine: Patient comfort and pain relief. Br J Anaesth.
- Wells CI, Xu W, Penfold JA, Keane C, Gharibans AA, et al. (2022) Wearable devices to monitor recovery after abdominal surgery: A scoping review. BJS Open 6: zrac031.
- Xu W, Karanicolas PJ, Eskicioglu C (2024) Feasibility and accuracy of wrist-worn sensors for perioperative monitoring. J Surg Res 290: 174-182.
- Gehl CJ, Verhagen NB, Shaik TJ, Nimmer K, Yang X, et al. (2024) Association of daily step count and postoperative complications among surgical patients. J Am Coll Surg 239: 539-546.
- Kondo S, Nakajima M, Kato H (2025) Postoperative step count predicts 90-day unplanned readmission after thoracic esophagectomy. Ann Surg Oncol 32.
- Ou-yang CL, Ma LB, Wu XD, Ma YL, Liu YH, et al. (2024) Association of sleep quality on the night of operative day with postoperative delirium in elderly patients: A prospective cohort study. Eur J Anaesthesiol 41: 226-233.
- Ryan T, Walker AM, Liepert D (2024) Discriminatory ability of perioperative heart rate variability in predicting postoperative complications in major urologic surgery: A prospective cohort study. Sci Rep 14: 11965.
- Wagoner CW, Thomas A, Dort JC, Sauro KM, Nelson G, Sauro KM (2025) Enhanced recovery after surgery compliance and outcomes for head and neck reconstructive surgery. JAMA Otolaryngol Head Neck Surg 151.
- Hazrati E, Eftekhar SP, Mosaed R, Dini SS, Namazi M (2024) Understanding the kynurenine pathway: A narrative review on its impact across chronic pain conditions. Mol Pain 20.
- Pocivavsek A, Schwarcz R, Erhardt S (2024) Neuroactive kynurenines as pharmacological targets: New experimental tools and therapeutic opportunities. Pharmacol Rev 76: 978-1008.
- Nelson MJ, Yu DA, Ha AVH, Wakefield MR, Fang Y (2025) Causes and effects of postoperative sleep disorders and treatment strategies across the perioperative, intraoperative, and postoperative settings-A narrative review. Clocks Sleep 7: 29.
-
- Shin HW, Lee JH, Lim J (2024) Effectiveness of perioperative melatonin on postoperative outcomes: A systematic review and meta-analysis of randomized controlled trials. J Int Med Res.
- Zhang X, Zheng J, Zhao Y (2024) Effect of transcutaneous auricular vagus nerve stimulation vs sham on chronic insomnia: A randomized clinical trial. JAMA Netw Open 7: e2451217.
- Shebl MA, El-Maghawry M, Khaled S (2025) Preoperative anxiety and its impact on surgical outcomes: A meta-analysis. J Perioper Pract.
- Gustafsson UO, Rockall TA, Wexner S, How KY, Emile S, et al. (2025) Guidelines for perioperative care in elective colorectal surgery: Enhanced recovery after surgery (ERAS) society recommendations-2025. Surgery 184.
- (2020) Perioperative care in adults. National Institute for Health and Care Excellence (NICE).
- Rafiq RB, Yount S, Jerousek S, Roth EJ, Cella D, et al. (2023) Feasibility of PROMIS using computerized adaptive testing during inpatient rehabilitation. J Patient Rep Outcomes 7: 44.
- (2018) Implementing patient-reported outcome measures in clinical practice: A companion guide to the ISOQOL user’s guide. ISOQOL.
- (2023) Patient-reported outcomes (PRO) FHIR implementation guide (R4, STU). HL7®.
- Habermann A, Widaeus M, Soltani N, Myles PS, Hallqvist L, et al. (2024) Days at home alive after major surgery in patients with and without diabetes: An observational cohort study. Perioper Med 13: 4.
- Irani JL, Hedrick TL, Miller TE, Lee L, Steinhagen E, et al. (2023) Clinical Practice Guidelines for Enhanced Recovery after Colon and Rectal Surgery from the American Society of Colon and Rectal Surgeons and the Society of American Gastrointestinal and Endoscopic Surgeons. Surg Endosc 37: 5-30.
- Barr E, Brannan GD (2024) Quality improvement methods (LEAN, PDSA, SIX SIGMA). StatPearls.
- (2025) Person-Centered Outcomes (PCO) FHIR implementation guide, 2024-2025. HL7 International.
- (2025) Collection and exchange of patient-reported outcomes. Interoperability Standards Advisory 2021. Office of the National Coordinator for Health Information Technology (ONC).
- Sreepada RS, Markin A, Shah SB (2023) Dashboard of short-term postoperative patient outcomes for anesthesiologists: Development and preliminary evaluation. Anesth Analg Pract Qual Saf.
- Sreepada RS, Chang AC, West NC, Sujan J, Lai B, et al. (2023) Dashboard of short-term postoperative patient outcomes for anesthesiologists: Development and preliminary evaluation. JMIR Perioper Med 6: e47398.
- Yoon SH, Ju JW, Lee HJ, Kim J, Kim MJ, et al. (2025) Development of the Korean enhanced recovery after surgery audit program Sci Rep 15.