Translational Perioperative and Pain Medicine (ISSN: 2330-4871)
ARTICLE DOI: 10.31480/2330-4871/179
Perspective | Volume 10 | Issue 3 Open Access
Steerable Intubation Guide in Combination with Video-Laryngoscope for Intubating Patients with Anterior Airway
Christian Bohringer, MD, Mathew Grow, MD and Hong Liu, MD*
Christian Bohringer, MD, Mathew Grow, MD and Hong Liu, MD*
Hong Liu, MD, FSAE, Department of Anesthesiology and Pain Medicine, University of California Davis Health, 4150 V Street, Suite 1200, Sacramento, CA 95817, USA, Tel: 916-734-5031, Fax: 916-734-7980, E-mail: hualiu@ucdavis.eduEditor: Renyu Liu, MD; PhD; Professor, Department of Anesthesiology and Critical Care, Perelman School of Medicine at the University of Pennsylvania, Center of Penn Global Health Scholar, 336 John Morgan building, 3620 Hamilton Walk, Philadelphia, PA 19104, USA, Fax: 2153495078, E-mail: RenYu.Liu@pennmedicine.upenn.edu
Received: July 16, 2023 | Accepted: October 23, 2023 | Published: October 26, 2023
Citation: Bohringer C, Grow M, Liu H. Steerable Intubation Guide in Combination with Video- Laryngoscope for Intubating Patients with Anterior Airway. Transl Perioper Pain Med 2023; 10(3):546-548
Abstract
Management of the difficult airway remains one of the most relevant and challenging clinical situations encountered by anesthesiologists. Intubation with a video-laryngoscope is often difficult in patients with anterior airway even when the larynx is readily visualized. This has led to the combined use of a video-laryngoscope together with a flexible bronchoscope for endotracheal intubation. The disposable flexible bronchoscopes that are currently available on the market however are not rigid enough to reliably guide the endotracheal tube into the larynx. A new steerable intubation guide is now available that is very useful when intubating a patient with an anterior airway with a video-laryngoscope.
Keywords
Difficult airway, Video-laryngoscope, Steerable intubation guide
Management of the difficult airway is still one of the most important and challenging clinical situations encountered by anesthesiologists in daily practice. It can develop into major adverse consequences if the airway is not secured in a timely fashion. Most airway problems can be solved with relatively simple devices and techniques, especially with video-laryngoscopes. However, clinical judgement and experience are crucial to their use. For any intubation technique, practice will improve performance and may reduce the likelihood of complications. Each airway device has unique properties that may be advantageous in certain situations yet limiting in others. Specific airway management techniques are greatly influenced by individual disease and anatomy, and successful management may require combinations of devices and techniques. The Video-laryngoscopes are now commonly used when intubating patients in the operating room (OR) [1]. There is one video-laryngoscope for every OR at our institution. When the indications for video-laryngoscopy are known neck instability, the potential for undiagnosed neck fracture, limited mouth opening or temporomandibular joint dysfunction, the stylet provided with the video-laryngoscope usually has the correct curvature to allow for easy intubation with the neck in the neutral position.
When trying to intubate a patient with an anterior airway and a short thyromental distance, however, the endotracheal tube (ETT) often cannot be steered successfully into the trachea using the standard stylet even though the video-laryngoscope provides adequate visualization of the vocal cords [2]. Changing to a video-laryngoscope with a D-blade can improve visualization of the vocal cords but does not make it any easier to steer the ETT into the trachea because it does not solve the fundamental problem that the oral, pharyngeal and laryngeal axes do not align when the neck is in the neutral position. In patients with anterior airway, the tip of the ETT first needs to be anteflexed to pass through the vocal cords and then must be retroflexed so that the ETT can be inserted deeply enough into the trachea to inflate the cuff. This can be accomplished by guiding the ETT into the trachea with the help of a flexible bronchoscope. This combined use of the video-laryngoscope to visualize the vocal cords and the flexible scope to steer the ETT into the trachea has become common practice when intubating patients with anterior airway anatomy [3,4]. The combined technique works well when utilizing a reusable flexible scope that has sufficient internal rigidity. Most of the disposable flexible scopes currently available on the market however do not have sufficient internal rigidity to reliably guide the ETT into the trachea. When trying to advance the ETT over these floppy disposable flexible scopes the ETT frequently pulls the disposable flexible scope out of the trachea. The flexible scope then forms a blind loop in the esophagus and fails to guide the ETT into the trachea. This blind loop phenomenon is encountered more often when the circumference of the flexible scope is too small for the diameter of the ETT. The external diameter of the flexible scope used as an intubation guide should be at least three quarters of the internal diameter of the ETT. Warming the ETT to reduce its stiffness or using a spirally reinforced ETT will also make it easier for the ETT to follow the flexible scope into the airway.
While current disposable scopes provide adequate visualization for bronchoscopy, they are poorly suited for steering an ETT during intubation. Health care organizations are however motivated to replace re-useable scopes with disposable scopes because re-useable endoscopy equipment continues to be implicated in nosocomial cross-contamination between patients [5]. A steerable intubation guide named QUICKSTEER TM (Access Airways, Blaine, MN) has recently become available. This intubation guide is very suitable to be used together with a video-laryngoscope because it has a steering function. When using a video-laryngoscope blade for intubation with the neck in the neutral position the oral, pharyngeal and laryngeal axes are not aligned as well as when employing a standard Macintosh blade with the patient in the “sniffing position”. Using a video-laryngoscope blade also does not create sufficient space in the oropharynx for effectively using Magill forceps to manipulate a conventional bougie. The ability to steer a bougie or intubation guide is therefore a great benefit in this situation.
The QUICKSTEER TM intubation guide needs to be lubricated well so that the ETT can slide over it easily. The current version allows use of ETTs down to size 6. The intubation guide needs be steered into the trachea by itself, and the handle then must be taken off before the ETT can be advanced over it. The video-laryngoscope blade should remain in the oropharynx until the ETT has been successfully placed in the larynx. This facilitates passing the ETT into the larynx and identifies any potential damage to the vocal cord during the intubation. The QUICKSTEER TM intubation guide cannot be used for nasal ETTs and the ETT cannot be preloaded onto the bougie because the currently available version is not long enough for that. The distance from the tip of the intubation guide to the handle is 30 cm while the length of a size 8.0 ETT including the connector is 34.5 cm. The total length of the intubation guide is 67 cm. Subsequent versions of this device may allow for nasal intubation by placing the handle at a greater distance from the tip (Figure 1 and Figure 2).
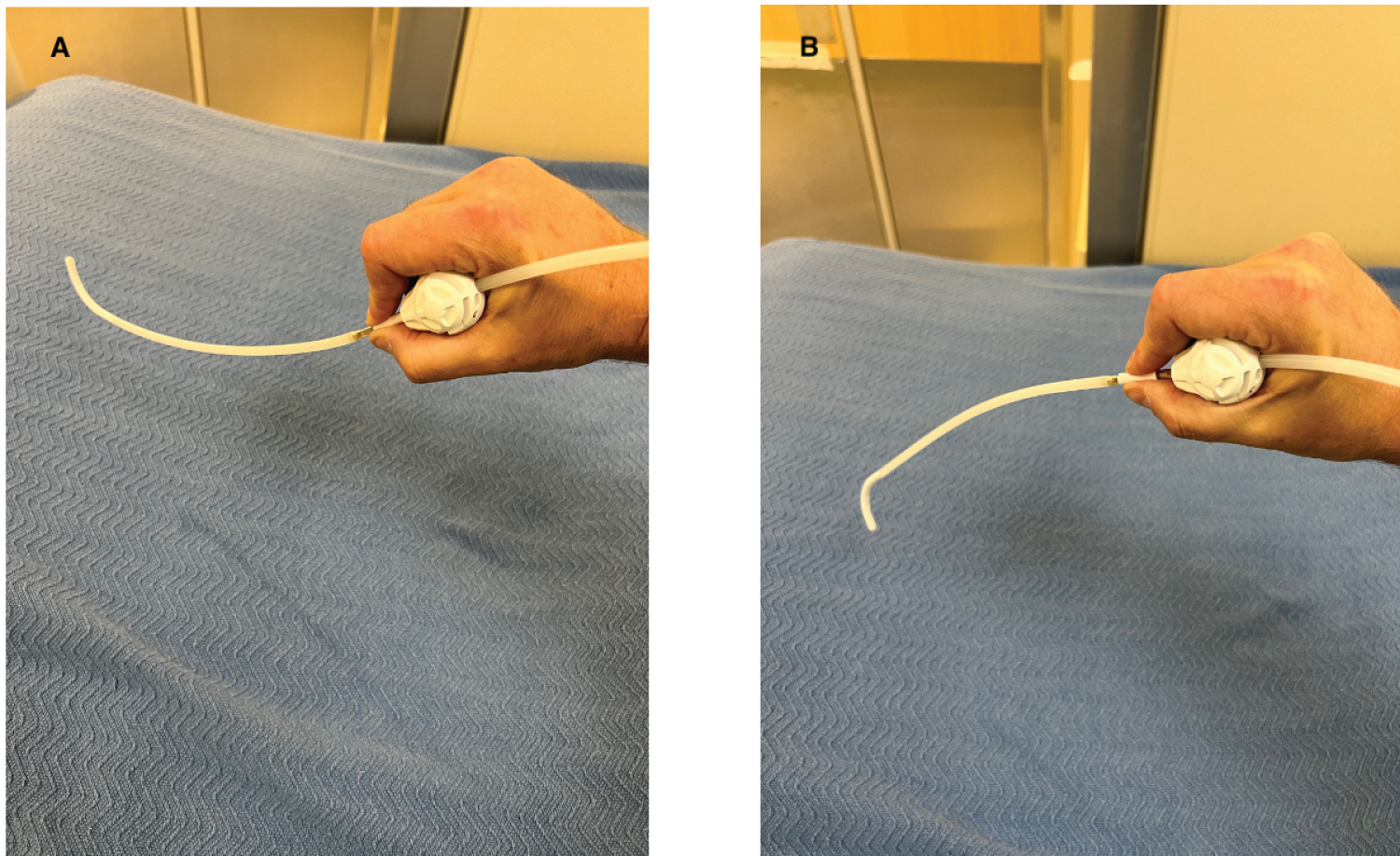
Figure 1: (A) The QUICKSTEERTM intubation guide is held by the handle and the actuator sleeve located below the handle is pinched between the right thumb and the index finger; (B) Pushing the sleeve away from the handle ante-flexes the tip of the intubation guide and pulling the sleeve towards the handle retro-flexes the tip. Left-right directional control is achieved by rotating the wrist.
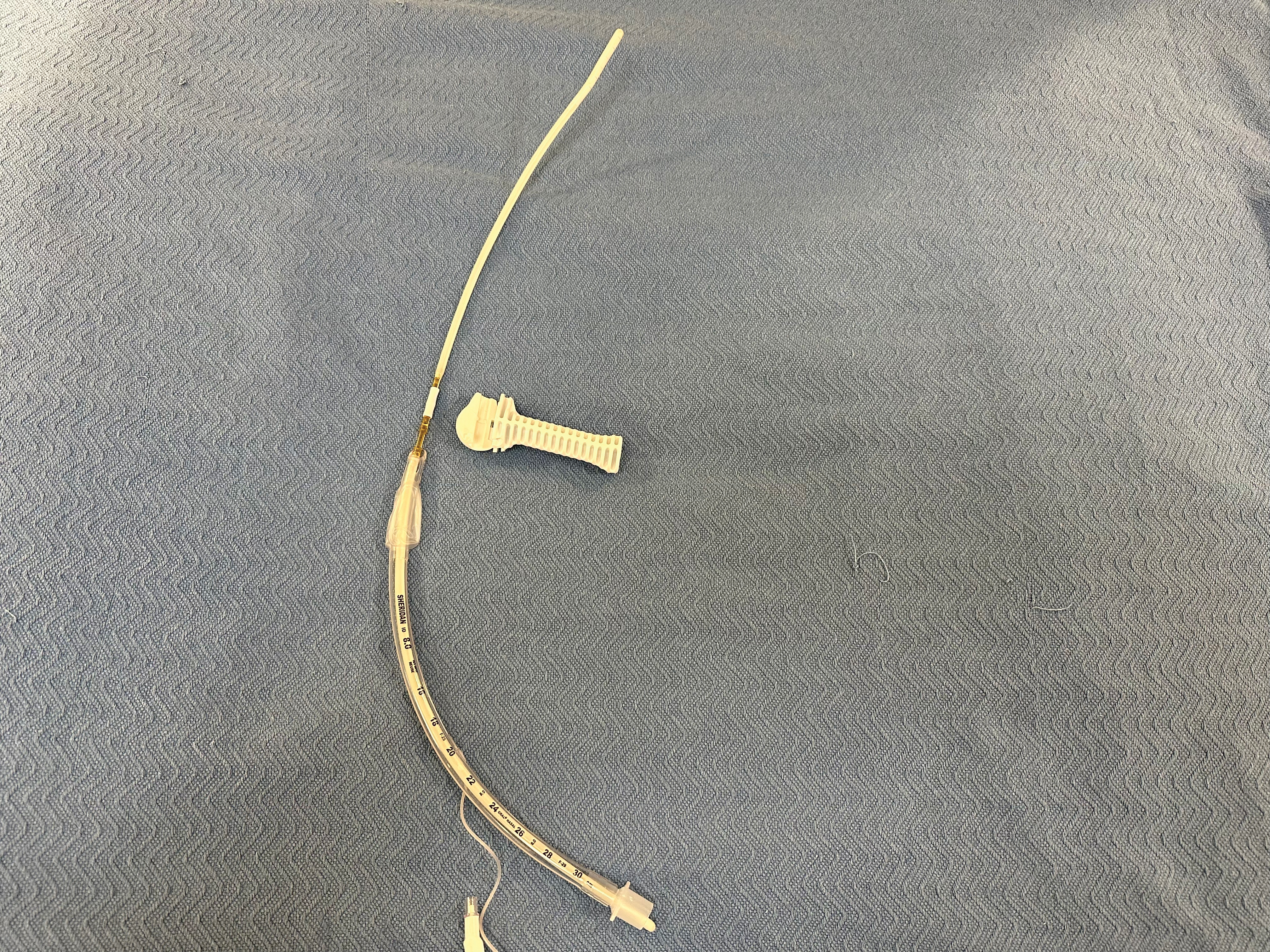
Figure 2: After the intubation guide has been inserted into the trachea the handle needs to be taken off so that the ETT can be advanced over it.
In summary, this new steerable intubation guide costs less than a disposable flexible scope and has greater internal rigidity. It can significantly facilitate intubation in a patient with an anterior airway when using a video-laryngoscope.
Funding
This work was supported by the Department of Anesthesiology and Pain Medicine, Department of Surgery and Department of Internal Medicine of University of California Davis Health System and NIH grant UL1 TR000002 of the University of California Davis Health.
Conflict of Interests
The author reports no conflict of interests.
References
- DI Marco P, Iannuccelli F. Videolaryngoscopes: Can we finally get the view around the corner? Minerva Anestesiol. 2016 Sep;82(9):926-8.
- Greenland KB, Segal R, Acott C, Edwards MJ, Teoh WH, Bradley WP. Observations on the assessment and optimal use of videolaryngoscopes. Anaesth Intensive Care. 2012 Jul;40(4):622-30. doi: 10.1177/0310057X1204000407.
- Bohringer C, Duca J, Liu H. A synopsis of contemporary anesthesia airway management. Transl Perioper Pain Med. 2019;6(1):5-16.
- Khan MF, Shamim F, Slote MU, Salim B, Abbas SA. Combined use of a videolaryngoscope and a flexible bronchoscope for awake tracheal intubation when front-of-neck airway is not an option. Anaesth Rep. 2021 Jan 13;9(1):12-15. doi: 10.1002/anr3.12091.
- Travis HS, Russell RV, Kovaleva J. Cross-contamination rate of reusable flexible bronchoscopes: A systematic literature review and meta-analysis. J Infect Prev. 2023 May;24(3):95-102. doi: 10.1177/17571774231158203.